
Challenges of designing pain management tech for kids

As a kid, when I’m at the dentist or getting treatment, I catch myself picking at my own skin to distract myself from the procedure. One time I even picked at it so hard it started bleeding. There are many reasons behind this small action, including how distraction can reduce the perception of pain. But instead of bleeding and hurting ourselves, is there a way to distract, and hopefully, make these bad moments a little more tolerable for kids?
Why does this matter?
Sometimes it’s not just a “be braver and suck through it” easy thing. Poorly managed procedural pain in children can lead to longer procedure times, the need for physical restraints, and increased distress for everyone in the room. The longer-term consequences matter too. Negative memories can amplify pain and fear at future visits (Noel et al., 2012), needle phobia can start developing (Chan, E. 2023), and that can lead to healthcare avoidance and vaccine hesitancy down the line.
To make the experience better for kids and parents, and to make clinicians’ work easier, designers and clinicians are collaborating to make the experience so engaging that the brain doesn’t have room to feel pain.
How distraction-based pain management works
Most of the tools are using two complementary ideas. The first is the gate control theory of pain (Melzack and Wall, 1965), which argues that non-painful sensory input can “close the gate” on pain signals traveling to the brain. When someone rubs a bumped knee, the rubbing activates nerve pathways that block pain signals in the spinal cord before they ever reach the brain (Cleveland Clinic). Same mechanism as rubbing a boo-boo.
The second idea emphasizes that pain is not a simple input-output system but a multidimensional experience shaped by attention, emotion, and context (Melzack, 2001). A child’s perception of a needle stick is connected to their anxiety about it, their memories of past procedures, and how much cognitive bandwidth they have available for the sensation. If something else is taking up that bandwidth, the brain might end up constructing less of a pain experience.
Each tool below uses one or both of these mechanisms to different degrees.
Buzzy device

Compared to the technologies introduced later, this one is a low-tech but effective device. The Buzzy device is a small, bee-shaped plastic gadget that applies simultaneous vibration and cold to the skin near a needle insertion area. The design turns a medical device into something more playful and intuitive. Inventor Dr. Amy Baxter designed it so that ice packs become “wings,” the vibration becomes a “buzz” (Kanchwala, 2014). You don’t need too much explanation, just put the bee on your arm, it buzzes, it’s cold, and the needle might hurt less.
Buzzy is a straightforward application of gate control: vibration and cold both add competing sensory input that interferes with pain signal transmission before it reaches the brain (Melzack & Wall, 1965). A 2025 systematic review and meta-analysis found that the Buzzy device had a statistically significant effect on reducing both pain and anxiety during needle-related procedures in children and adolescents.
Social robots

Robots offer a physical, social presence. Something that talks, moves, and responds in the room with the child. Unlike Buzzy, social robots don’t block pain signals at the sensory level. They work on the cognitive-emotional side. A 2025 study describes how a socially assistive robot was designed to serve different roles across phases of a procedure: before, providing emotional support and education; during, delivering distraction and coaching coping; after, offering praise and comfort. A systematic review and meta-analysis found that, during needle-related procedures in children, robot-based distraction reduced anxiety and distressed avoidance behaviors compared to standard care, though the difference in pain scores was not statistically significant.
Virtual Reality
VR is where both mechanisms work at once. On the gate control side, VR floods the visual and auditory channels with so much sensory input that there’s less capacity for pain signals to get through. On the cognitive-emotional side, it creates what researchers call “presence,” the feeling of actually being in the virtual world. A 2026 systematic review found that VR distraction significantly reduced pain scores compared to control conditions in pediatric emergency department settings, and research on presence suggests this sense of immersion is a key reason VR outperforms simpler distractions like blowing bubbles or watching cartoons.
However, not all VR content works equally. A 2025 HCI study on VR gamification for post-surgical children found that action and shooter-style games were most effective at reducing pain, while RPGs showed the least effect. Fast, reactive interactions that demand constant attention seem to leave the brain very little bandwidth left to process pain.
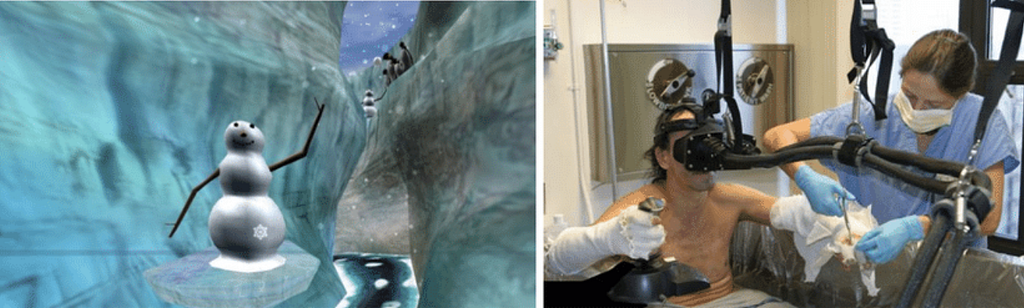
SnowWorld, designed for burn wound care, is a good example of these principles in practice. Children throw snowballs at snowmen and mammoths in an icy canyon, a deliberate choice by creator Hunter Hoffman, who designed it as ‘the antithesis of fire’ to keep burn patients’ minds away from the flames. The interaction is simplified to match the user’s condition: locomotion is automatic, and the only input is pointing your head and clicking a button to throw. Hoffman noted that these are patients in pain and on medication, so the task had to be engaging enough to hold attention but easy enough that a sedated child could do it.
Augmented Reality
AR uses a different approach. Instead of shutting out the real world, it reframes the context. Stanford’s CHARIOT program has introduced AR headsets that show animated avatars demonstrating the process of IV placement while the child watches their own procedure happening. The shift, from “I don’t know what’s happening to me” to “I can see what’s happening and it’s okay,” directly addresses the anxiety, fear, and sense of helplessness that amplify pain perception. A systematic review found that AR captures children’s attention and improves the experience in the hospital, with evidence of pain reduction and reduced anxiety.
Is it practical, though?
All of these technologies sound promising. But clinical reality is very different from lab settings. There are technically three users in the room: the child who needs distraction, the parents who need reassurance, and the clinician who is time-pressed. I’ve heard clinicians say that no matter how effective a tool is, if it can’t be integrated into existing schedules and routines, it won’t get used. During busy flu season, no one is spending time setting up a VR headset, calibrating, and sanitizing between patients. There’s no single tool that fits all scenarios, and pros and cons need to be weighed carefully every time.
Procedure matters
Time is the biggest factor in choosing the right tool. Burn wound care (debridement, dressing changes, skin stretching) can take 20 to 45 minutes or more of sustained pain (Summer et al., 2007). That’s where VR makes the most sense. There’s enough time to put on a headset, settle into the experience, and maintain immersion throughout. SnowWorld was designed specifically for this, and similarly, longer procedures like chemotherapy port access (Gerçeker et al., 2020), MRI scans (Ryu et al., 2017), or physical therapy sessions (Won et al., 2017) give the technology room to work.
A routine blood draw is a different story. A child about to get shots sometimes only has seconds before the needle goes in, with no time for a tutorial or narrative buildup. And physically, interacting with VR controllers or gesturing in mid-air doesn’t work when a nurse needs the child’s arm still while trying to find the vein. For quick procedures, lower-tech options like Buzzy may be more practical.
The novelty problem
Most clinical trials involve single-session or short-term use. But what about kids with chronic conditions like cancer patients needing regular port access, burn patients facing weeks of dressing changes? Does the distraction effect hold up the 5th time? The 50th? This is largely unanswered. A 2025 study on parents’ perspectives on VR for pediatric chronic pain found that while parents saw strong potential, they highlighted concerns about sustained engagement and recommended that future VR technologies offer customizable content and adaptable experiences. More broadly, researchers have suggested that features like progression systems, rewards, and adjustable difficulty levels could help sustain engagement across repeated sessions. (Zhao et al., 2025).
Clinician communication and design tradeoff
When you fully immerse a child in VR, you cut off their awareness of the environment. Clinicians can’t easily say “hold still,” can’t explain what’s about to happen, and can’t read the child’s face for signs of distress. Some clinicians find it hard to work on a patient who is perceptually somewhere else. AR partially addresses this by keeping the real world visible, but at the cost of reduced immersive power, which might make it less effective as a distraction. The right tool to use depends on the procedure, the clinician’s comfort level, and the individual child’s needs.
Who gets left out?
Not all children can use VR headsets. Kids with certain neurological conditions, visual impairments, sensory processing disorders, or facial injuries may be excluded. But beyond those specific cases, there are issues that affect kids broadly. Most VR headsets aren’t designed for children’s smaller heads. The interpupillary distance settings often can’t adjust small enough for young eyes, which can cause eye strain, headaches, and blurred vision. The headsets are also heavy relative to a child’s body, putting strain on their neck and back.
The American Academy of Pediatrics recommends that children under 6 should not use VR at all because their sense of balance and visual systems are still developing. Research has also found that children’s developing eyes may absorb higher doses of radiofrequency radiation from VR devices than adults’ do. And cybersickness, the nausea and dizziness caused by a mismatch between visual motion and physical stillness, is another concern. Younger children are less likely to recognize or report when something feels wrong, which makes it harder to catch early.
Technology-based pediatric pain distraction is no longer just experimental; it’s actively used across major children’s hospitals. For example, Lucile Packard Children’s Hospital Stanford became one of the first hospitals in the US to implement VR distraction therapy across its patient units, covering emergency, oncology, orthopedics, and more. Shriners Children’s Texas in Galveston has been using SnowWorld for burn patients since the mid-2000s, making it one of the longest-running clinical applications of VR pain distraction.
While the overall direction of research is positive, gaps still exist. Most evidence is concentrated on acute procedural pain. The case for chronic pain management is far less developed. A review published in early 2026 found that many individual studies have small sample sizes, use inconsistent hardware and content, and lack blinding. The field is moving toward multimodal pain management, combining distraction technology, parental coaching, and child life specialist support to cover ground that no single tool can on its own. With more research on maintaining effectiveness over repeated use and integrating these broader approaches, hopefully these tools can become more accessible and helpful to every child who needs them.
Design for pain: how to make the worst moment better was originally published in UX Collective on Medium, where people are continuing the conversation by highlighting and responding to this story.