
Design challenges and limitations for VR addiction treatment

Addiction is a chronic, relapsing condition, and most people who struggle with it cycle through multiple rounds of treatment before achieving lasting recovery. However, stigma keeps many people from seeking care in the first place, and even those who do often relapse when they leave the therapist’s office and re-enter the world of bars, parties, casinos, and street corners where their habits were built.
Some researchers are trying to address the gap between clinic and real world with Virtual Reality. In December 2025, Texas Health became one of the first health systems in the Dallas-Fort Worth area to integrate VR into routine addiction care, letting patients practice managing triggers in simulated parties, bars, and family gatherings under therapist supervision. Their platform is also one of the few that incorporates olfactory elements, introducing scents like synthetic marijuana, vodka, or beer to deepen the immersive experience. This kind of program also raises some design questions. What should the virtual environment include to make the treatment effective? How do skills built inside the headset transfer to real life? And what does success even look like, both for the clinicians and the patients?
How does this work?
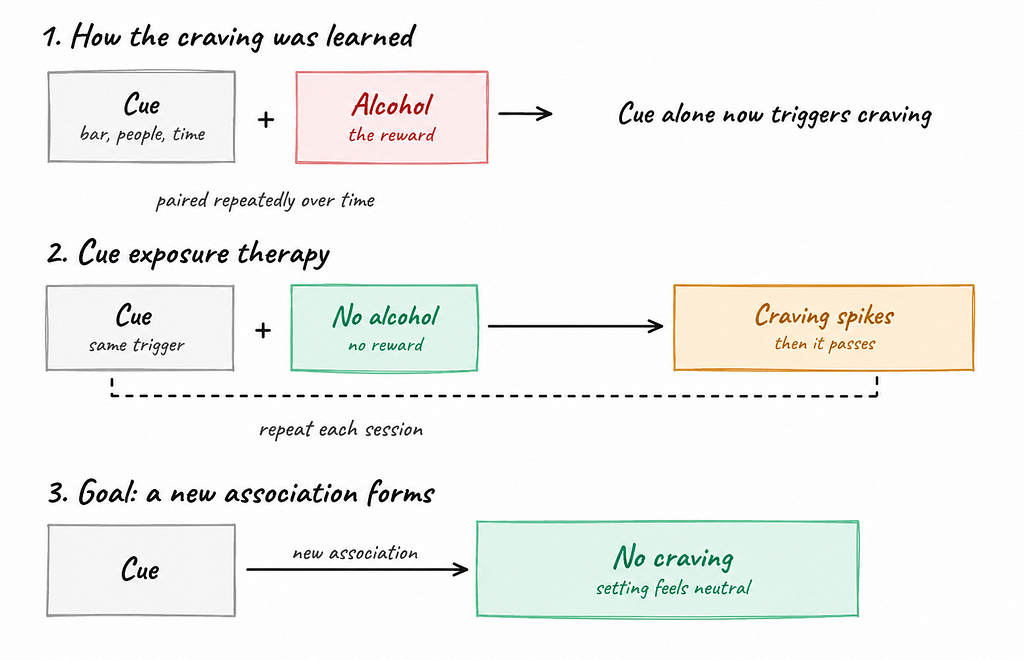
In some cases, when someone uses a substance over and over, their brain pairs the substance with the settings where they take it, whether that’s a particular bar, certain people, a specific time of day, or a familiar emotional state. Over time, those neutral surroundings turn into conditioned cues that can set off a craving even without the substance anywhere in sight.
Patients are sometimes treated with Cue Exposure Therapy (CET). The idea is to deliberately put the patient in front of those cues in a safe, controlled space, over and over. The craving gets triggered on purpose. However, nothing follows it, no high, just the urge passing on its own, again and again, and gradually a new association forms. This means that, ideally, those settings won’t trigger the patient’s craving in the real world anymore. Since craving intensity is an important predictor of relapse, reducing craving could be an effective tool for relapse prevention. Creating a convincing environment for this kind of therapy can be challenging. With VR, a clinician can build a realistic, engaging environment with personalized cues, and do it all from inside a treatment room.
Even though the whole idea sounds promising, the research shows mixed results. It helps to think of VR as doing two separate jobs. The first is triggering craving in a controlled setting, and VR does that well. In one study, smokers placed in virtual scenarios experienced measurable craving responses, with those who later relapsed showing especially strong reactions. The second job of VR treatment is keeping people clean months down the line, and that’s where things get harder. A 2025 research tested VR-CET as an add-on to standard smoking cessation therapy in 246 participants. At six months, people relapsed at roughly the same rates whether they got VR-CET or an active relaxation control (progressive muscle relaxation). The skills used to calm a craving inside a session haven’t reliably translated into staying sober weeks and months afterward.
What’s the challenge?
Several factors contribute to that gap. Some are personal, some are technical, and some are tied to the treatment system itself. Below are just some of them:
Select the right cues
Knowing what sets off a particular person’s craving is hard, and sometimes the trigger is something the patient isn’t even aware of. Craving is deeply personal. It’s been shaped over years by which substance someone used, the social situations they used it in, and the emotions associated with using. A virtual bar that triggers one patient’s craving might do nothing for another. Building environments varied enough to catch the right cues for each patient is challenging.
Provide complete sensory experience
Even though some programs, like the one at Texas Health, incorporate synthetic scents, most still rely heavily on vision and audio. Sight and sound are easy to recreate, but other senses like smell, touch, and taste are not. Some of the most powerful relapse triggers are exactly the ones that VR can’t easily create, such as the smell of cigarettes or the physical presence of a specific person.
Clinical workflow and usability
These sessions have to be run under a clinician’s guidance. A 2022 feasibility study across three inpatient addiction clinics showed that acceptability was high among both patients and therapists, and both groups advocated for VR use. However, barriers still existed. Clinicians needed time, training, and confidence with the technology before they could use it well. What really decided whether VR got used wasn’t how much patients enjoyed it but practical things like whether it was easy to operate, whether staff got proper training and tech support, and whether it actually fitted the clinical workflow.
Over-reliance on VR simulations
Skills that someone learned in a virtual bar may not carry over to a real one. This is a known limitation of extinction learning called the renewal effect, in which craving reduction stays tied to the setting where you achieved it and can come back when the person hits the same cue somewhere new. However, research also shows potential fixes: bringing along a reminder from the treatment setting, like a specific object or routine, can help the learned calm stick. Other practical fixes include mixing up the cues and changing the environment across sessions so the brain doesn’t tie its progress to just one setting.
VR treatment isn’t designed to be used alone. Effective treatment still relies on things like therapy, medication, and peer support. VR is just a tool that makes some of that work easier, more flexible, and more realistic. Designing for VR addiction treatment can be challenging. It isn’t just about making the most immersive headset experience. It’s about picking the right cues, building a workflow that actually fits a clinician’s day, and giving the patient something they can carry out of the headset and into real life.
Reference:
Texas Health Resources. (2025, December). Reality Check: How Texas Health is Using Virtual Reality in the Treatment of Addiction. https://www.texashealth.org/newsroom/News-Releases/2025/Reality-Check-How-Texas-Health-is-Using-Virtual-Reality-in-the-Treatment-of-Addiction
ScienceDirect. Cue Exposure. Background on classical conditioning and cue exposure in addiction. https://www.sciencedirect.com/topics/psychology/cue-exposure
Thaysen-Petersen, D., Hammerum, S. K., Düring, S. W., Larsen, P. V., Fink-Jensen, A., & Mellentin, A. I. (2025). The efficacy of conventional and technology assisted cue exposure therapy for treating substance use disorders: A qualitative systematic review. Frontiers in Psychiatry, 16, 1544763. https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2025.1544763/full
Vafaie, N., & Kober, H. (2022). Association of drug cues and craving with drug use and relapse: A systematic review and meta-analysis. JAMA Psychiatry, 79(7), 641–650. https://pubmed.ncbi.nlm.nih.gov/35648415/
Liao, Z., et al. (2025). Virtual reality-based cue exposure therapy reduces psychological craving in men with methamphetamine use disorder: A randomized controlled trial. Translational Psychiatry, 15, 318. https://www.nature.com/articles/s41398-025-03553-7
Schröder, B., Kroczek, A., Kroczek, L. O. H., Ehlis, A.-C., Batra, A., & Mühlberger, A. (2024). Cigarette craving in virtual reality cue exposure in abstainers and relapsed smokers. Scientific Reports, 14, 7538. https://www.nature.com/articles/s41598-024-58168-7
Batra, A., et al. (2025). Virtual reality cue exposure as an add-on to smoking cessation group therapy: A randomized controlled trial. Addiction Science & Clinical Practice, 20, 34. https://link.springer.com/article/10.1186/s13722-025-00561-2
Markus, W., et al. (2022). Virtual reality to support inpatient addiction treatment: Patients are ready, what about therapists? A feasibility study. International Journal of Mental Health and Addiction, 21(6), 4085–4107. https://link.springer.com/article/10.1007/s11469-022-00843-9
Bouton, M. E. (2002). Context, ambiguity, and unlearning: Sources of relapse after behavioral extinction. Biological Psychiatry, 52(10), 976–986. https://doi.org/10.1016/S0006-3223(02)01546-9
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., & Vervliet, B. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. https://doi.org/10.1016/j.brat.2014.04.006
Can VR treat addiction? was originally published in UX Collective on Medium, where people are continuing the conversation by highlighting and responding to this story.